
Research Article | DOI: https://doi.org/10.31579/2578-8868/196
1*Intituto Nacional de Neurología y Neurocirugía (INN). La Habana Cuba
2Centro Internacional de Restauración Neurológica (CIREN). La Habana, Cuba.
1Intituto Nacional de Neurología y Neurocirugía (INN). La Habana Cuba
1Intituto Nacional de Neurología y Neurocirugía (INN). La Habana Cuba
3Instituto Nacional de Higiene, epidemiologia y microbiología (INHEM)
4Instituto Pedro Kouri (IPK). La Habana, Cuba.
1Intituto Nacional de Neurología y Neurocirugía (INN). La Habana Cuba
5Texas Woman’s University, Department of Ph.D. Studies, Denton, TX, USA
*Corresponding Author: Santos Santos Aise, Intituto Nacional de Neurología y Neurocirugía (INN). La Habana Cuba
Citation: Aisel S. Santos., Morales Chacón LM., Narjara C. Ferrán., Dearriba Romanidy MU., Liana P. Hernández., et all. (2021) Factors Associated with Short-Term Seizure Recurrence in Extratemporal Epilepsy Surgery. J. Neuroscience and Neurological Surgery. 9(3); DOI:10.31579/2578-8868/196
Copyright: © 2021 Santos Santos Aise, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 14 July 2021 | Accepted: 29 July 2021 | Published: 04 August 2021
Keywords: extratemporal epilepsy surgery; prognosis, predictors
Introduction: Drug-resistant extratemporal epilepsy is the second cause of referral to epilepsy surgery.
Objectives: To identify factors associated with short-term seizure recurrence following extratemporal epilepsy surgery.
Materials and Methods: We performed a retrospective study of 19 consecutive patients who underwent surgery for drug-resistant extratemporal epilepsy at the National Institute of Neurology and Neurosurgery of Havana, Cuba, from September 2014 to October 2019. All patients had at least one year of postoperative follow-up. Fisher's exact test was used to search for an association between dichotomous variables. A value of p≤0.05 was considered significant.
Results: After one year of follow-up, seizure freedom reached 31.6% (Engel I) and 36.8% showed significant improvement in the number of seizures (Engel II). The frontal location (p=0.046) and incomplete resection of the epileptogenic zone (p=0.017), bilateral interictal discharges on the preoperative electroencephalogram (EEG) (p=0.017), the presence of epileptiform discharges on the postsurgical EEG (p=0.001), and the occurrence of seizures after the sixth month of surgery (p=0.001), were associated with seizures recurrence.
Conclusions: After one year, 31.6% of patients operated on for extratemporal epilepsy were seizure-free. The incomplete resection of the epileptogenic zone and the presence of epileptogenic discharges in the postsurgical EEG, and the presence of seizures after the sixth month of surgery were the most significant factors of seizure recurrence.
Estimations consider that at least 50 million people live with epilepsy worldwide, 5 million of whom are from the "Americas".[1] Close to one-third of cases do not respond to pharmacological treatment, and of these, between 10 and 15% are candidates for surgery. [2]
20% of patients who underwent surgery showed the extratemporal location, predominantly in the frontal lobe. [3, 4] The outcomes of different series of extratemporal surgery are varied. West et al.(5)found 30 to 50% of seizure freedom (Engel I), Morales et al. [6], in Cuba, found 52.6% of patients in Engel I during the first year and 41.1
We performed a retrospective study of 19 consecutive patients operated for drug-resistant extratemporal epilepsy at the National Institute of Neurology and Neurosurgery of Havana from September 2014 to October 2019, with a comprehensive epilepsy surgery program. All the patients had at least one year post-surgery follow-up.
The information was gathered from the patients’ medical records. The variables evaluated as potential predictors were: a) age at diagnosis of epilepsy and at the time of surgery; b) medical history (initial precipitating factors related to epilepsy in the prenatal, perinatal, or postnatal stage); c) seizure semiology and monthly frequency; d) preoperative electroencephalogram (interictal EEG, ictal onset) and neuroimaging findings; e) type of surgery; f) results of intraoperative electrocorticography (ECoG) before and after surgery; g) anatomopathological studies; h) postoperative electroencephalogram (EEG) and magnetic resonance imaging (MRI) as well as i) the occurrence of seizures before and after six months. [4-7, 9]
Preoperative evaluation [6,10]
All patients were evaluated in a non-invasive way, with prolonged video-EEG monitoring and electrodes placed according to the international 10-20 system and additional electrodes depending on the topography of the epileptogenic zone (EZ). The interictal epileptiform activity was classified as ipsilateral whenever it was consistent with the ictal onset or bilateral zone when it occurred in both hemispheres. 1.5T and/or 3T high-field MRI with epilepsy protocol was performed in all patients and interictal and ictal single-photon emission tomography (SPECT) was co-registered to MRI in patients with normal MRI.
Surgical Procedure
Depending on the type of surgical procedure used, these were classified as resection, disconnection, or a combination of both. [5]A pre-surgical ECoG was performed and patterns were classified as specific, according to criteria based on Boonyapisit 2003: a) isolated spikes, amplitude> 200 mV; b) bursts duration> 0.5 s, amplitude> 200 μV, frequency ±7–10 Hz, regular firing; c) paroxysmal fast: burst duration> 0.5 s, frequency> 10 Hz, regular firing and d)runs of slow repetitive spikes: duration> 0.5 s, amplitude> 200 μV, frequency <7>
Postoperative prognosis and follow-up [10]
Anatomopathological studies of the samples were performed and classified as focal cortical dysplasia (FCD) according to the ILAE classification, (12) descriptive or unspecified.
Six months after surgery, an MRI was performed. It was evaluated whether the resection of the estimated epileptogenic zone (EZ) was complete or incomplete. It was considered a complete resection when it was possible to completely resect the identified ictal area and the cortex that showed epileptiform activity on EcoG. In patients in whom the MRI showed a lesion, a total resection of said lesion guided by ECoG with the absence of epileptiform activity at the edges of the resection. An EEG was also performed to analyze the topography and the presence or absence of epileptiform activity. After the first year, the cases were classified according to the Engel Class Outcome System, Engle I was considered a good prognosis (seizure freedom) and Engel II to IV a recurrence of seizures, short-term follow-up (one year). [4,7]
Statistical analysis
The information was stored in a Microsoft Excel database, and its analysis was carried out in the SPSS system version 20.1.
The categorical variables were presented in the form of frequencies and percentages. Fisher's Exact Test was used to associate the dichotomous variables. A value of p≤0.05 was considered significant.
Ethical aspects
This research was approved by the Institute of Neurology and Neurosurgery Ethics Committee, which acted following the current laws and regulations issued by the Ministry of Public Health of Cuba (MINSAP) and follows the principles outlined in the Declaration of Helsinki of the World Medical Association for Human Medical Research.
Of the 19 patients studied, 16 were male and three females, ranging in age between 13 and 34 years. Most of them (57.9 %) were distributed in the age group of 16 to 30 years.
After one year of follow-up, 31.6 % of the patients were seizure-free (Engel I), seven patients (36.8 %) presented significant seizure improvement (Engel II). The rest were distributed between Engel III (21.1%) and Engel IV (10.5%).
It was observed a predominance of patients with over 15 years from the time of their epilepsy diagnosis until surgery with 13 patients (68.4 %), 8 of which (42.1 %), with more than 20 years of evolution of their disease. (Table 1)

Focal-onset seizures with impaired awareness were the most frequent, 16 patients (84.2 %); likewise, 16 presented seizures with evolution to a bilateral tonic-clonic at some point in their disease. 57.9% of the cases presented more than 20 monthly seizures before surgery. None of these variables was statistically associated with postoperative evolution.
Patients with a history such as hypoxia and head trauma (6 patients = 31.6%) were distributed on the Engel II scale upwards.
The ictal onset in the frontal lobe predominated, 13 patients (68.4%), 11 presented recurrence of seizures. Both had a statistical association in the short term.
Interictal epileptiform activity occurred bilaterally in 8 patients (42.1 %), all of them presented recurrence of seizures after surgery, which was statistically associated (p = 0.017).
On MRI, 57.9% of the patients presented lesions, primarily distributed between Engel I and II. Six non-lesional patients underwent ictal and interictal SPECT and subsequent co-registration with MRI. The focal hyperperfusion found in all of them was consistent with the rest of the evaluation.
Electrocorticography was performed in 16 patients (84.2%), who predominantly were classified as Engel I and Engel II, with classic patterns in the presurgical ECoG and the prevalence of the pattern of the repetitive spikes (68.4%). Table 2.
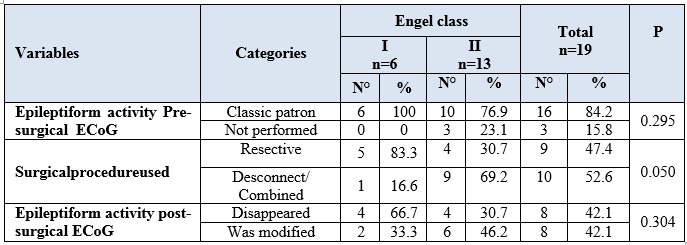
Resective surgical techniques were given preference, 9 patients for a 47.4 %, prevailing the ECoG-guided lesionectomy, six patients (31.6 %), and subtotal lobar resections. Six patients (31.6 %) benefited from the combination of resective and disconnective techniques. Disconnection surgery was used in only four patients: anterior corpus callosotomy in three patients and multiple subpial transections (MST) in one patient with ZE in the primary motor area.
The postsurgical ECoG showed that the presurgical pattern disappeared in 8 patients (42.1%), and in other 8 patients it was modified.
The most frequent anatomopathological diagnosis was the focal cortical dysplasia type IA with six patients (31.6 %), distributed across Engel classes II to IV, followed by FCD IIA. Out of those that evolved without seizures after surgery (Engel I), two patients were classified as FCD type III B (associated with tumors) and two patients as descriptive results.
In the postsurgical EEG, 11 patients (57.9 %) presented interictal epileptiform discharges (IED), all presented recurrence of seizures after surgery (Engel II-IV), which was statistically significant (p = 0.001). Table 3
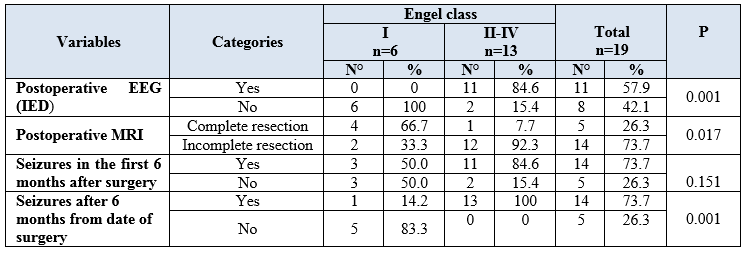
Patients with incomplete resection of the EZ (73.7%) predominated in class II or higher of the Engel scale (seizure recurrence), finding a statistical association between these variables (p = 0.017).
Of the 14 patients who presented seizures six months after surgery, 13 evolved from Engel II to Engel IV, which was statistically significant (p = 0.001).
Regarding the postoperative complications, the evolution was very favorable, with a low rate of complications related to the surgical procedure in 4 patients (21.1%), a cingulate infarction, 2 cerebrospinal fluid fistulas, and an epidural hematoma.
In the present research, most cases were male, and the prevailing age group that of 16 to 30 years. Other studies show similar data, such as one that was carried out in China [13] with 82 patients operated on for frontal lobe epilepsy, male sex predominated (59.8%), and the mean age was 19.1 years. Similarly, in a meta-analysis carried out in Cincinnati, USA, with 2028 patients, the male sex predominates (54.3 %), and the mean age is 10.24 ± 1.11 years.[14] Similar results were found in the Cuban series of Morales et al.[6] with 55% male predominance and a mean age of 24.1 ± 10.1 (ranging 5 - 47 years).
The 2019 Cochrane review, [5] reports 30 to 50% seizure freedom after extratemporal epilepsy surgery. In another investigation of frontal lobe surgery, [4] seizure freedom is obtained in 45%, 34%, 26%, 20% and 14% at the end of the 1st, 2nd, 3rd, 4th and 5th years respectively after the surgery. Morales et al. [6], in Cuba, find 52.6 % of the patients in Engel I in the 1st year and 41.1
A small sample that reduces the possibility of generalizing the results from the statistical point of view.
The frontal location of the epileptogenic zone and its incomplete resection, the bilateral interictal activity in the presurgical EEG, interictal epileptiform discharges in the postsurgical electroencephalogram, and the presence of seizures after the sixth month after surgery was statistically associated with seizure recurrence.
A favorable evolution was obtained in more than half of the cases, grouped into the Engel classes I and II.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
